בית > Reconstructive surgeries > Fractures in the eye socket
Fractures in the orbit mainly result from blunt trauma (falls, car accidents, bullet wounds, fights). The most common fracture is called a Blowout fracture and results from a fracture in the lower wall of the orbit (the floor of the orbit, towards the maxillary sinus, inferior orbital wall) as well as in the medial wall towards the nose (medial wall), there is usually a prolapse of the orbit contents (fat/muscle) into the sinus. The clinical symptoms are swelling and bleeding, exudates in the eyelids with decreased sensation in the lower eyelid area up to the lower lip. These usually pass within a few days to weeks. Double vision accompanied by restriction of movement, especially when looking up, is very typical. When there is no significant restriction in the movement of the eyeballs, there is no urgency for surgery to repair the fracture, and it is possible to wait a week to several weeks. In extensive fractures, surgery can be considered to prevent the eye from sinking in (enophthalmos). In cases where there is muscle entrapment in the fracture area, the patient will usually experience nausea, vomiting, and significant difficulty opening the eyes. In this case, surgery should be performed as soon as possible to prevent further damage to the muscle. A fracture with true entrapment is characteristic of children or young adults, and is called a white-eyed blowout fracture because it is usually not accompanied by bleeding in the eyelids. In any case of injury to the orbit (dark and/or sharp), orbital imaging (CT) should be performed to examine the presence of a fracture and to rule out intraorbital foreign bodies.
Pre-surgery photos:


Diagnosis of orbital fracture is made based on the clinical history of a blunt trauma to the orbital cavity and according to the examination findings: swelling and hemorrhages around the eyes, limitation of eyeball movement accompanied by double vision, lack of sensation in the lower eyelid and cheek area up to the upper lip, and sometimes air in the subcutaneous tissue (orbital emphysema). When there is a high clinical suspicion of an orbital fracture and/or nausea, vomiting, and inability to open the eyes, it is recommended to perform a computed tomography of the orbital cavities, CT, thin sections including coronal reconstructions to confirm the diagnosis of the fracture. In the absence of suspicion of an intraorbital foreign body, a CT scan can be performed without contrast material. The CT scan clearly demonstrates the presence of a fracture in the orbital walls.
Other types of chimney fractures include a fracture of the lateral wall of the jaw joint (ZMC) and a fracture of the nasal bone (NOE).
It is important to know that most orbital fractures do not require surgery; small fractures tend to heal spontaneously without clinical disturbance over time. When there is an extensive fracture in the orbital floor or medial wall, a sunken eye may gradually develop after several months due to the prolapse of orbital fat into the fracture space. If the sunken eye is aesthetically disturbing, surgery may be considered. Additional indications for surgery include significant limitation of movement that does not resolve after 2-4 weeks, as well as entrapment of the inferior rectus muscle with a white-eyed blowout fracture, especially with an oculo-cardiac reflex (slow pulse, nausea, vomiting, and inability to open the eye). The latter case requires urgent intervention as soon as possible to prevent long-term damage to the muscle. The absence of sensation or the presence of air in the soft tissues around the eye is not an indication for surgery.
Most oculoplastic surgeries are performed by an oculoplastic surgeon with expertise in oculoplastics. When there is jaw involvement, or a fracture of the nasal bone, if surgery is required, it will be performed in conjunction with an oral and maxillofacial specialist and an otolaryngologist.
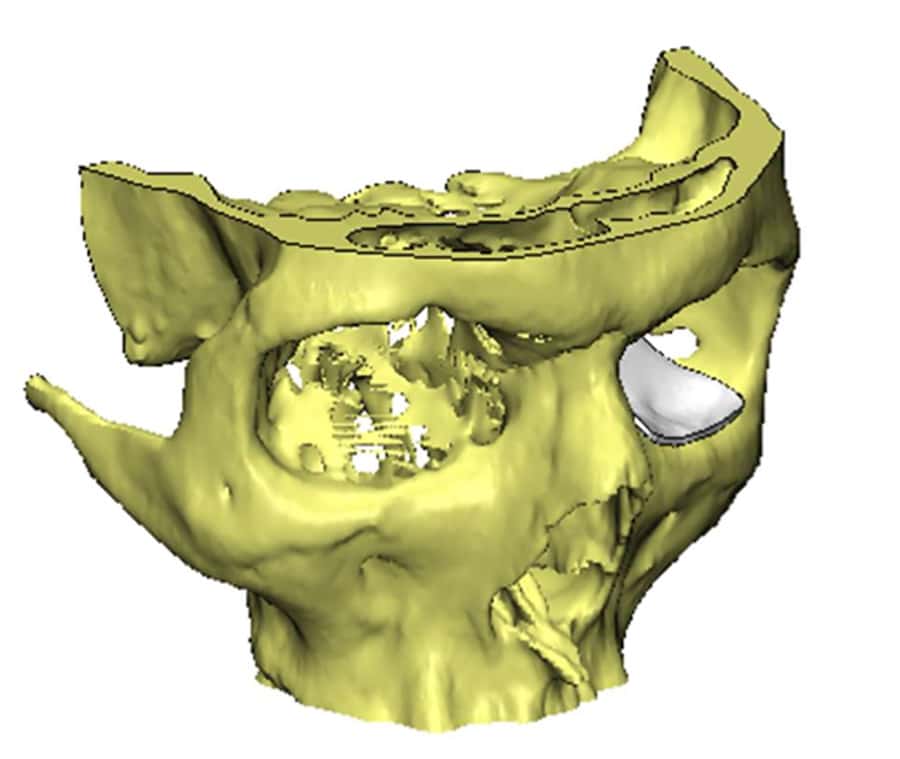
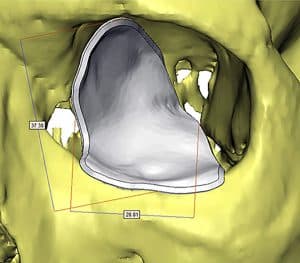
In surgery to repair a fracture in the floor of the orbit and the medial wall, it is common to return the contents of the orbit that have fallen into the nasal cavities, and to place an alloplastic surface at the borders of the fracture in order to prevent further prolapse. There are many types of implants, most of which are made of titanium with a combination of a coral-like plastic material (porous polyethylene). Today, there are implants that are customized according to the dimensions of the fracture, and they are printed or designed according to the computed tomography scan – patient preferred implants PPI. In a large study, we compared the results of repairing an orbital fracture with customized implants, and we found that in cases of extensive complex fractures, there may be a significant advantage to using this implant .
In cases of fractures in children with incarceration of the inferior rectus muscle, it is not necessary to place an implant if the fracture is trap door and there is no significant prolapse of the contents of the nasal cavity tissue into the nasal cavities.
The surgery is performed through the inner side of the eyelid (a hidden incision through the conjunctiva), usually with a small incision at the corner of the eyelids. During the surgery, the fracture area is exposed, and the tissue that has fallen into the nasal cavities is returned to the chimney. A plastic material or titanium mesh is placed in place of the fracture in order to restore volume to the chimney. In cases where there are foreign bodies within the chimneys and their removal does not endanger the eye, chimney surgery can be performed to remove the foreign body.
In certain cases, Prof. Ben-Simon uses custom -made implants according to the size of the fracture, the imaging image, and the structure of the uninvolved socket.
The surgical technique is called ORIF – open reduction internal fixation, since the uvula is not a major weight-bearing organ. The technique is based on restoring as much of the prolapsed uvula tissue as possible, covering all the fracture boundaries with the implant, if necessary, fixing the implant with titanium screws, and finally suturing the conjunctiva and reconstructing the eyelid angle.
In the first few days, there is pain in the chimney accompanied by swelling and subcutaneous hemorrhage. Sometimes there may be restriction of movement and even double vision that will pass within a few days to weeks. Numbness in the area of the fracture can last for several months and in most cases passes spontaneously.
Full recovery from the surgery occurs 2-3 months after the operation, at which time the degree of success of the surgery and the degree of functional and aesthetic improvement can be assessed. If a sunken eye remains with aesthetic disturbance, or residual limitation of movement, surgery with the placement of an additional implant, a customized implant, or strabismus correction surgery can be considered. The percentage of repeat surgeries is not common.
If there is no significant limitation of movement, and the fracture is not extensive according to the imaging test, there is no urgent indication for surgery. You can wait a few weeks, assess improvement, and if necessary, decide on surgery. It is important to remember that most fractures in the eye sockets heal spontaneously and do not require surgery.
Likewise, even if the clinical examination is normal, and there is a history of dark trauma to the socket, it is not necessarily recommended to perform an imaging test. Today, the amount of radiation in computed tomography of the eye sockets is not high, but of course, if possible, it is better to avoid it.
The absence of sensation or numbness in the lower eyelid, cheek, and upper lip in the presence of a chimney fracture is a fairly common phenomenon. It occurs because the sensory nerve is almost always located near the fracture area. In most cases, the phenomenon gradually disappears after a few weeks. This phenomenon may also appear or worsen after surgery to repair the chimney fracture, and here too, it usually disappears spontaneously.
Double vision after a chimney floor fracture is usually due to edema in the innervation of the muscles that move the eyeball. In most cases, the double vision gradually resolves in the weeks following the injury as the edema resolves. Double vision can be monitored and measured with strabismus tests or the HESS eye movement test. If the double vision does not resolve, refractive surgery, prism glasses, or strabismus correction surgery can be considered.